Medicare has quietly built the first federal payment program designed for AI agents — and most of the technology industry has no idea it exists. The Medicare ACCESS model, which goes live on July 5, 2026, creates a reimbursement structure that for the first time makes AI-driven chronic care economically viable inside the U.S. healthcare system. If you build, fund, or operate in health tech, this is the policy change you’ve been waiting for.
What Is the Medicare ACCESS Model?
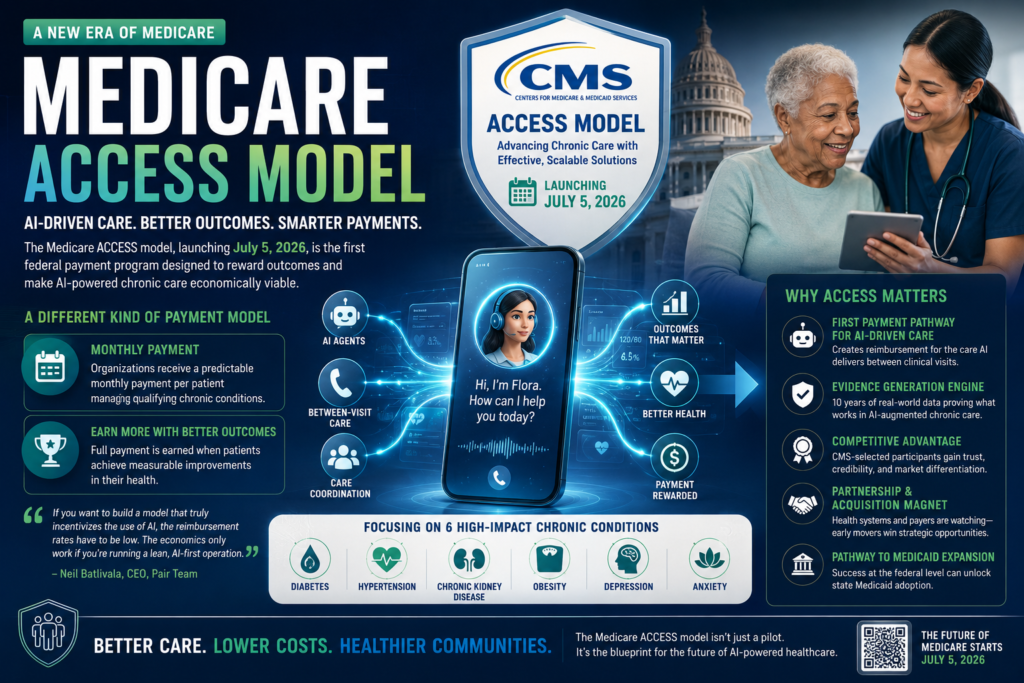
Definition: The Medicare ACCESS model — formally titled Advancing Chronic Care with Effective, Scalable Solutions — is a 10-year program operated by the Centers for Medicare & Medicaid Services (CMS) that tests a payment structure rewarding health outcomes rather than clinical activities.
Expansion: Under this program, participating organizations receive a predictable monthly payment for managing qualifying chronic conditions. They earn the full amount only when patients achieve measurable health improvements: lower blood pressure, reduced pain scores, better glycemic control. The covered conditions are diabetes, hypertension, chronic kidney disease, obesity, depression, and anxiety — six of the most prevalent chronic illnesses driving Medicare spending.
The program launched with 150 participating organizations selected by CMS from a competitive applicant pool. Participants range from AI-first clinical startups to virtual nutrition therapy providers, connected device companies, and wearable hardware manufacturers.
What makes the program structurally significant is who designed it. Abe Sutton, Director of the CMS Innovation Center, previously worked as a venture capitalist at a healthcare fund. Jacob Shiff, the Center’s Chief AI and Technology Officer, is a former healthcare founder. Both joined CMS under the Trump administration, and their startup backgrounds are directly visible in ACCESS’s design: outcome-based payments, direct-to-consumer enrollment pathways, and an explicit mandate for competition between participants.
Why Traditional Medicare Cannot Support AI-Driven Care
Question: Why can’t existing Medicare billing codes accommodate AI-powered care?
Direct Answer: Because Medicare has always paid for clinician time — and AI doesn’t have a billing code.
There is currently no federal reimbursement mechanism for an AI agent that monitors a patient between office visits, conducts a check-in call, coordinates a housing referral, or verifies that someone has picked up a prescription. These activities happen outside the clinical encounter, which is precisely where AI systems operate most effectively — and where traditional Medicare payment is completely silent.
This isn’t a bureaucratic oversight. It reflects the underlying structure of fee-for-service billing, which was designed around a legible, auditable unit: a physician sees a patient, documents the encounter, submits a claim. That unit maps cleanly to an in-person visit. It does not map to a voice AI agent conducting an hour-long intake call with a patient living out of their car.
The result is a fundamental misalignment. The clinical interventions most likely to improve health outcomes — between-visit check-ins, care coordination calls, social needs navigation — are precisely the interventions that traditional Medicare will not pay for. AI-driven care doesn’t generate a billing event under the existing system.
CMS’s new program creates that mechanism for the first time. It doesn’t pay for specific activities. It pays for outcomes. That distinction is the entire logic of the shift.
How the ACCESS Program Transforms AI Healthcare Economics
This program is not simply a new reimbursement rate. It is a structural transformation of the incentive environment — one that, for the first time, makes AI-first healthcare operations economically rational at scale.
The Payment Logic That Makes AI Work
Under traditional fee-for-service Medicare, the economics of AI integration are difficult to justify. Adding an AI agent to a clinical workflow generates additional cost and complexity without producing additional billing events. The AI agent’s work is invisible to the payment system — it can improve outcomes but cannot be captured as revenue.
Under the ACCESS program, the economics invert. Organizations receive a fixed monthly payment per enrolled patient and retain more of it when outcomes improve. The only way to expand margins within that reimbursement structure is to reduce the per-patient cost of delivering care — which means automation. Pair Team CEO Neil Batlivala articulated this logic directly: “If you want to build a model that truly incentivizes the use of AI, the reimbursement rates have to be low. The economics only work if you’re running a lean, AI-first operation.”
This is deliberate policy design, not a funding constraint.
Traditional Medicare vs. the ACCESS Model: A Side-by-Side Comparison
| Feature | Traditional Fee-for-Service Medicare | CMS ACCESS Program |
|---|---|---|
| Payment basis | Per clinical encounter (visit, procedure) | Monthly per-patient payment for managed conditions |
| AI agent reimbursement | None — no billing code exists | Implicitly supported via outcome-based structure |
| Incentive direction | More volume = more revenue | Better outcomes = full payment retention |
| Between-visit care | Not reimbursed | Central to the program’s care model |
| Patient enrollment method | Clinician-initiated | Direct-to-consumer enrollment permitted |
| Program duration | Status quo | 10-year pilot starting July 2026 |
| Method flexibility | Rigid coding requirements | Outcome-defined, method-agnostic |
What “Outcome-Based” Actually Means in Practice
The phrase “value-based care” has been used loosely in health policy for over a decade. What distinguishes ACCESS is the specificity and enforceability of its outcome requirements. Participants don’t show they’re trying to manage patients well — they demonstrate measurable improvements on the six covered conditions to receive full payment. Organizations that enroll patients without moving their health metrics will earn reduced reimbursement. This is not a pay-for-participation model.
Who Is in ACCESS and What They’re Actually Building
The Participant Landscape
The first ACCESS cohort reflects the breadth of current health tech investment: AI-powered clinical operations platforms, virtual-first primary care practices, connected device companies using continuous monitoring hardware, and consumer wearable brands including Whoop. Neil Batlivala expressed skepticism about some participants’ fit with the ACCESS population. “I’m a big fan of wearables, but for a senior who’s struggling with food insecurity, I don’t know how much Whoop is going to be able to do,” he said.
The populations CMS designed this program to serve are not typical early adopters of digital health tools. They are older, lower-income patients managing multiple chronic conditions, often alongside unstable housing, food scarcity, and limited transportation. Organizations that have built specifically for this population have a structural advantage over those arriving from consumer health.
Pair Team and Flora: A Deep Case Study in AI-Driven Care
The clearest current illustration of AI-powered chronic disease management under this kind of payment model is Pair Team, a California-based company founded in 2019. Pair Team built its model specifically for patients managing chronic illness alongside social determinants of health — the non-medical factors like housing and food access that are among the strongest predictors of outcomes.
The company employs roughly 850 clinical professionals, operates what it describes as the largest community health workforce in California, and generates over nine figures in annual revenue. It has raised approximately $30 million, backed by Kleiner Perkins, Kraft Ventures, and Next Ventures.
About nine months before the ACCESS announcement, Pair Team deployed a voice AI agent named Flora as its primary patient-facing interface. Flora is available 24 hours a day. It handles patient intake, coordinates referrals to housing and food programs, and conducts the between-visit check-ins that keep patients engaged with their care plans.
The results have been meaningful. A peer-reviewed study co-authored by Pair Team researchers, published in the Journal of General Internal Medicine, evaluated the company’s community-integrated care model. The study found strong patient engagement and significant reductions in avoidable emergency and inpatient utilization. Internally, the company reports that one in four hospital visits and one in two ER visits don’t occur when a patient is in its program.
The human dimension of Flora’s work is illustrated by a specific call Batlivala described. A 67-year-old woman living out of her car, managing PTSD and congestive heart failure, spoke with Flora for over an hour. He described the call as both remarkable and sobering — Flora may have been the only conversation she’d had in weeks about her situation. Hour-long interactions have since become routine. “That’s the companionship piece,” he said. “And it turns out that is truly an intervention.”
Pair Team currently has partnerships giving it access to roughly 500,000 potential patients, with a goal of reaching one million within three years.
The Real Risks: Data, Finances, and an Uncertain Track Record
Intellectual honesty requires acknowledging the genuine risks of the ACCESS program alongside its structural promise.
Data Privacy for Vulnerable Populations
ACCESS participants collect extraordinarily sensitive patient information: intimate conversations about housing instability, mental health diagnoses, and chronic illness histories. This data flows through federal infrastructure with a documented history of security problems, including past incidents involving exposed Social Security numbers. For the low-income, chronically ill patients the program is designed to serve, a data breach isn’t an abstract inconvenience — it can affect housing applications, insurance eligibility, and personal safety. The vulnerability of this population makes data protection not just a compliance requirement but an ethical obligation.
The CMS Innovation Center’s Mixed Track Record
The CMS Innovation Center, which administers ACCESS, does not have a straightforward success record. A 2023 Congressional Budget Office analysis found the Center increased federal spending by $5.4 billion during its first decade rather than delivering projected savings. That history raises legitimate questions about whether the 10-year pilot will achieve its stated goals — or whether it will demonstrate that well-designed payment models are harder to execute at scale than they appear on paper.
The Reimbursement Math Is Tight
CMS is paying less per patient per month than many ACCESS participants anticipated. Several organizations entering the program expected rates that would allow a gradual transition to AI-augmented care. Instead, the rates are structured so that the economics only work for organizations that have already automated the majority of patient interactions. For participants who haven’t yet scaled their automation infrastructure, the first year may be financially difficult.
What This Means for Health Tech Founders and Investors
The Medicare ACCESS model is the first federally-designed payment framework that explicitly rewards AI-first operations in chronic disease management. For the health technology sector, the implications run across investment thesis, product strategy, and go-to-market planning.
Key Opportunities the ACCESS Program Creates
- A reimbursement pathway for AI agents. For the first time, organizations can build revenue models around care that AI systems deliver between clinical visits. The between-visit interaction gap — previously unbillable — becomes the core value proposition.
- An evidence-generation engine. Ten years of outcome data under consistent payment rules will produce the most rigorous real-world comparison yet between AI-augmented and traditional chronic disease management. Early participants accumulate proprietary evidence that strengthens future positioning with payers, health systems, and acquirers.
- Regulatory validation as a competitive signal. Acceptance into the program represents CMS evaluation and selection from a competitive applicant pool. Participation in the Medicare ACCESS model is a credible signal of clinical and operational maturity — one that is difficult for later entrants to replicate.
- A partnership and acquisition magnet. Large health systems and insurers are watching ACCESS participants closely. Many are unwilling to build AI-first care models internally. Early participants gain visibility with potential partners and acquirers at the moment those organizations are beginning to evaluate their strategic options.
- A template for Medicaid expansion. If ACCESS demonstrates cost savings at the federal level, it creates evidentiary and political momentum for analogous programs in state Medicaid systems — potentially doubling the accessible patient population for companies that have proven their model.
- Increased demand for enabling infrastructure. Voice AI platforms, care coordination software, social determinants data integrations, and outcome measurement tools are all prerequisites for operating effectively under the ACCESS payment structure. Infrastructure companies in these categories benefit from rising demand as the ACCESS cohort scales.
Digital health funding hit its highest Q1 total since the COVID-19 pandemic in early 2026, with AI-focused companies capturing the majority of new capital. The ACCESS program gives that capital a deployment thesis that has not previously existed in federal healthcare payment policy.
What Founders Should Evaluate Before Applying
Not every AI health company is positioned to succeed under the ACCESS structure. The economics require a lean, highly automated operation. Organizations that rely heavily on human care teams for routine patient interactions may find that reimbursement rates are insufficient to cover costs.
Before pursuing an ACCESS application, founders should evaluate the following:
- What percentage of patient interactions currently require human staff versus automated systems?
- Can the organization’s cost structure support ACCESS reimbursement rates while maintaining care quality standards?
- What peer-reviewed or audited evidence exists of outcome improvement for the six ACCESS-covered conditions?
- How does the organization currently handle data security for sensitive patient communications at scale?
Companies that cannot answer those questions confidently are likely to face financial pressure in the program’s first year.
The Bottom Line: Why the Medicare ACCESS Model Matters for AI Healthcare
The Medicare ACCESS Model is not just another healthcare pilot program hidden inside government policy language. The Medicare ACCESS Model is a structural shift in how chronic care can be funded, delivered, measured, and scaled across the United States. For years, healthcare founders, AI startups, and investors have all faced the same frustrating problem: even if AI could improve patient outcomes, there was no reimbursement system designed to support that work. The Medicare ACCESS Model changes that equation.
At its core, the Medicare ACCESS Model introduces a payment framework that rewards results instead of activities. Traditional Medicare has historically paid providers for appointments, procedures, tests, and documented clinician time. That structure made sense in a healthcare system built around hospitals and in-person care. But it was never designed for AI-powered chronic care management. An AI agent checking in with a diabetic patient, reminding them about medication adherence, or helping schedule transportation to a clinic generates value but not a billable event. Under old rules, that work was economically invisible.
This is exactly why the Medicare ACCESS Model matters. The Medicare ACCESS Model finally recognizes that healthcare does not begin and end inside a doctor’s office. Chronic care happens every day, between appointments, inside homes, through patient behavior, lifestyle choices, and ongoing engagement. The Medicare ACCESS Model creates a monthly reimbursement pathway that makes these interventions financially viable.
For health tech founders, the Medicare ACCESS Model is effectively a green light from CMS. The government is signaling that AI-driven care is no longer a futuristic experiment—it is now a reimbursable healthcare category. That single policy shift could accelerate the next decade of digital health innovation. Companies that previously struggled to monetize AI care coordination, remote patient engagement, or voice-based chronic care now have a potential federal payment mechanism through the Medicare ACCESS Model.
The long-term implications are significant. If the Medicare ACCESS Model proves that AI-first care organizations can improve outcomes for diabetes, hypertension, chronic kidney disease, obesity, depression, and anxiety while lowering costs, then the model could influence far more than Medicare. A successful Medicare ACCESS Model could become the blueprint for Medicaid expansion programs, private insurer reimbursement strategies, and future CMS innovation initiatives.
Investors should also pay close attention. The Medicare ACCESS Model reduces one of the biggest risks in digital health investing: reimbursement uncertainty. In the past, many promising AI healthcare startups had strong products but weak business models because there was no sustainable payer pathway. The Medicare ACCESS Model introduces a clearer revenue logic. Startups that can automate patient engagement, improve outcomes, and manage chronic disease efficiently now have a stronger case for scale.
That said, optimism should come with caution. The Medicare ACCESS Model is not guaranteed success. The CMS Innovation Center has a mixed history, and previous pilots have failed to generate the projected savings policymakers promised. The reimbursement math inside the Medicare ACCESS Model is intentionally tight, meaning only highly efficient organizations with strong automation capabilities are likely to thrive. Companies relying too heavily on human-heavy operations may struggle under this framework.
Data privacy is another critical issue. The Medicare ACCESS Model requires participants to handle extremely sensitive patient information, including mental health conditions, financial instability, housing insecurity, and medication histories. As AI systems become more integrated into care delivery, the success of the Medicare ACCESS Model will depend not only on cost savings and clinical outcomes, but also on trust, compliance, and ethical data governance.
Still, despite these challenges, the strategic importance of the Medicare ACCESS Model is difficult to overstate. The healthcare system has spent years discussing value-based care in theory. The Medicare ACCESS Model operationalizes that concept in a way specifically aligned with AI-driven care delivery.
The biggest takeaway is simple: the Medicare ACCESS Model creates a new swim lane for healthcare innovation. Founders no longer have to force AI into reimbursement systems built for physician time. Instead, the Medicare ACCESS Model rewards organizations for achieving what healthcare should have prioritized all along—better patient outcomes.
Whether the first cohort succeeds or fails, the significance of the Medicare ACCESS Model remains intact. CMS has formally acknowledged that AI can play a legitimate operational role in chronic disease management. That recognition alone is historic.
The Medicare ACCESS Model may still be a pilot, but it is arguably the clearest signal yet that the future of healthcare reimbursement is shifting toward automation, outcomes, and scalable chronic care management. For health tech builders, operators, and investors, ignoring the Medicare ACCESS Model now would be like ignoring cloud computing in its early days—possible, but probably not wise.